2017-03-19 07:33:02
Prelude
Today's topic(s)
- Depression
Depression
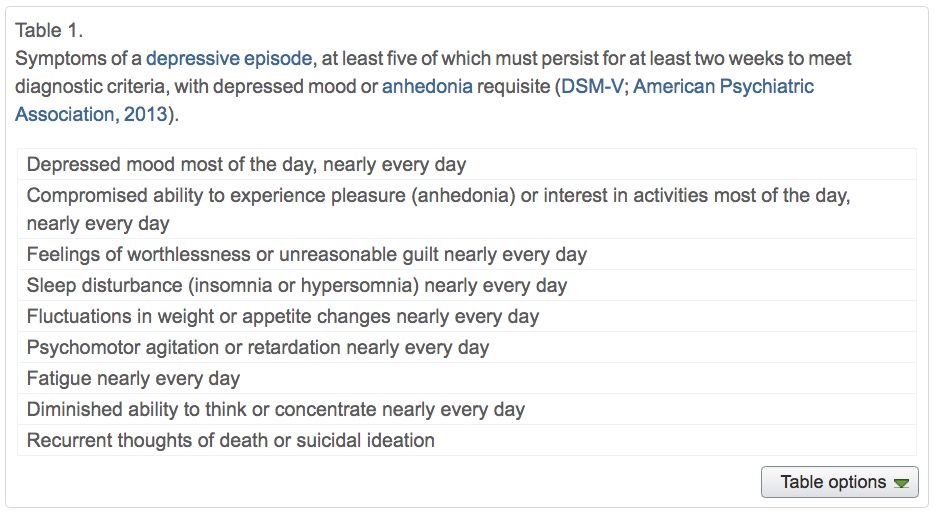
- Symptoms
- Unhappy mood, insomnia, lethargy, loss of pleasure, interest, energy
- Agitation
- Lasting for several weeks or more
Depression
- Experienced by ~7% Americans in any year
- Prevalence (up to ~20% lifetime)
- Females 2-3x males, higher 40+ years of age
- MZ concordance ~60% vs. DZ ~20% suggests genetic component
Symptoms, (Mahar et al. 2014)
Neurological factors
- Reduced hippocampal volumes
- (Videbech and Ravnkilde 2004) meta-analysis
- Meta-analysis combines effects across many different studies
(Videbech and Ravnkilde 2004)

(Videbech and Ravnkilde 2004)

Neurological factors
- Hypoactivity in
- Frontal and temporal cortex
- Anterior cingulate
- Insula
- Cerebellum
- (Fitzgerald et al. 2008)
(Fitzgerald et al. 2008)

- patients v. controls, (b) patients on SSRIs, (c) patients v. ctrls (happy stim), (d) patients v. controls (sad stim)
Neurological Factors
- Persistent activation in amygdala
- Amygdala and dorsolateral prefrontal cortex (DLPFC) inversely related
- (Siegle et al. 2002)
Disrupted connectivity
- Resting state fMRI (rsFMRI) in 421 patients with major depressive disorder and 488 control subjects.
- Reduced connectivity between orbitofrontal cortex (OFC) and other areas of the brain
- Increased connectivity between lateral PFC and other brain areas


Disturbed sleep
- Less slow wave (stage 3 and 4)
- More REM earlier in night (typical is longer REM as night goes on)

Pharmacological factors
- Endocrine
- Lowered thyroid function
- High/chronic cortisol levels
Pharmacological factors
- Monoamine hypothesis
- More: euphoria
- Less: depression
- Resperine (antagonist for NE & 5-HT) can cause depression
- Low serotonin (5-HT) metabolite levels in CSF of suicidal depressives (Samuelsson et al. 2006)
(Samuelsson et al. 2006)

Treatments for depression
- Psychotherapy
- Often effective when combined with drug treatment
- Drugs
- Exercise
Drugs
- Monoamine oxidase (MAO) inhibitors
- MAO destroys excess monoamines in terminal buttons
- MAO-I’s boost monoamine levels
- Tricyclics
- Inhibit NE, 5-HT reuptake
- Upregulate monoamine levels, but non-selective = side effects
Drugs
- Selective Serotonin Reuptake Inhibitors (SSRIs)
- Fluoxetine (Prozac, Paxil, Zoloft)
- Prolong duration 5-HT in synaptic cleft
- Also increase brain steroid production
- Selective Serotonin Norepinephrine Reuptake Inhibitors (SNRIs)
Cymbalta (SNRI)
How well do the drugs work?
- STAR*D trial
- On SSRI for 12-14 weeks. ~1/3 achieved remission; 10-15% showed symptom reduction.
- If SSRI didn't work, could switch drugs. ~25% became symptom free.
- 16% of participants dropped out due to tolerability issues
- Took 6-7 weeks to show response.
Who will benefit from drug therapy?
- Depends on
- Early life stress
- Brain (amygdala) response to emotional faces
- (Goldstein-Piekarski et al. 2016)
- Low-stress + low amyg reactivity -> > responding
- High stress + high amyg reactivity -> > responding

Problems with monoamine hypothesis
- Too simplistic
- NE, 5-HT interact
- Drugs fast acting (min), but improvement slow (weeks)
What do drugs do, then?
- Receptor sensitivity altered?
- Serotonin presynaptic autoreceptors compensate
- Postsynaptic upregulation of NE/5-HT effects
- Stimulate neurogenesis?
- Link to neurotrophin, brain-derived nerve growth factor (BDNF)
- BDNF boosts neurogenesis
- SSRIs stimulate new neurons in hippocampus
Exercise as a treatment

Drugs vs. therapy

(DeRubeis, Siegle, and Hollon 2008)

(DeRubeis, Siegle, and Hollon 2008)

(DeRubeis, Siegle, and Hollon 2008)

Electroconvulsive Therapy (ECT)
- Last line of treatment for drug-resistant depression
- Electric current delivered to the brain causes 30-60s seizure.
- ECT usually done in a hospital's operating or recovery room under general anesthesia.
- Once every 2 - 5 days for a total of 6 - 12 sessions.
Electroconvulsive Therapy (ECT)
- Remission rates of up to 50.9% (Dierckx et al. 2012)
- Seems to work via
- Anticonvulsant (block Na+ channel or enhance GABA function) effects
- Neurotrophic (stimulates neurogenesis) effects
Patients speak
- Kitty Dukakis' story: http://www.nytimes.com/2016/12/31/us/kitty-dukakis-electroshock-therapy-evangelist.html

Neurogenesis hypothesis, (Mahar et al. 2014)
- Chronic stress causes neural loss in hipp
- Chronic stress downregulates 5-HT sensitivity
- Depression ~ chronic stress
- Anti-depressants may upregulate neurogenesis via 5-HT modulation
Depression's widespread impact
- Widespread brain dysfunction
- Prefrontal cortex, amygdala, HPA axis, circadian rhythms
- Genetic + environmental factors
- Disturbance in 5-HT, NE systems, cortisol
- Many sufferers do not respond to available treatments
References
Babyak, Michael, James A Blumenthal, Steve Herman, Parinda Khatri, Murali Doraiswamy, Kathleen Moore, W Edward Craighead, Teri T Baldewicz, and K Ranga Krishnan. 2000. “Exercise Treatment for Major Depression: Maintenance of Therapeutic Benefit at 10 Months.” Psychosomatic Medicine 62 (5). LWW: 633–38. http://journals.lww.com/psychosomaticmedicine/Abstract/2000/09000/Exercise_Treatment_for_Major_Depression_.6.aspx.
Cheng, Wei, Edmund T. Rolls, Jiang Qiu, Wei Liu, Yanqing Tang, Chu-Chung Huang, XinFa Wang, et al. 2016. “Medial Reward and Lateral Non-Reward Orbitofrontal Cortex Circuits Change in Opposite Directions in Depression.” Brain, October, aww255. doi:10.1093/brain/aww255.
DeRubeis, Robert J., Greg J. Siegle, and Steven D. Hollon. 2008. “Cognitive Therapy Versus Medication for Depression: Treatment Outcomes and Neural Mechanisms.” Nature Reviews Neuroscience 9 (10): 788–96. doi:10.1038/nrn2345.
Dierckx, Bram, Willemijn T Heijnen, Walter W van den Broek, and Tom K Birkenhäger. 2012. “Efficacy of Electroconvulsive Therapy in Bipolar Versus Unipolar Major Depression: A Meta-Analysis.” Bipolar Disorders 14 (2): 146–50. doi:10.1111/j.1399-5618.2012.00997.x.
Fitzgerald, Paul B., Angela R. Laird, Jerome Maller, and Zafiris J. Daskalakis. 2008. “A Meta-Analytic Study of Changes in Brain Activation in Depression.” Human Brain Mapping 29 (6): 683–95. doi:10.1002/hbm.20426.
Goldstein-Piekarski, Andrea N., Mayuresh S. Korgaonkar, Erin Green, Trisha Suppes, Alan F. Schatzberg, Trevor Hastie, Charles B. Nemeroff, and Leanne M. Williams. 2016. “Human Amygdala Engagement Moderated by Early Life Stress Exposure Is a Biobehavioral Target for Predicting Recovery on Antidepressants.” Proceedings of the National Academy of Sciences 113 (42): 11955–60. doi:10.1073/pnas.1606671113.
Mahar, Ian, Francis Rodriguez Bambico, Naguib Mechawar, and José N. Nobrega. 2014. “Stress, Serotonin, and Hippocampal Neurogenesis in Relation to Depression and Antidepressant Effects.” Neuroscience & Biobehavioral Reviews 38 (January): 173–92. doi:10.1016/j.neubiorev.2013.11.009.
Samuelsson, M., J. Jokinen, A.-L. Nordström, and P. Nordström. 2006. “CSF 5-HIAA, Suicide Intent and Hopelessness in the Prediction of Early Suicide in Male High-Risk Suicide Attempters.” Acta Psychiatrica Scandinavica 113 (1): 44–47. doi:10.1111/j.1600-0447.2005.00639.x.
Siegle, Greg J., Stuart R. Steinhauer, Michael E. Thase, V. Andrew Stenger, and Cameron S. Carter. 2002. “Can’t Shake That Feeling: Event-Related fMRI Assessment of Sustained Amygdala Activity in Response to Emotional Information in Depressed Individuals.” Biological Psychiatry 51 (9): 693–707. doi:10.1016/S0006-3223(02)01314-8.
Videbech, Poul, and Barbara Ravnkilde. 2004. “Hippocampal Volume and Depression: A Meta-Analysis of Mri Studies.” American Journal of Psychiatry 161 (11). Am Psychiatric Assoc: 1957–66. doi:10.1176/appi.ajp.161.11.1957.